
OAB Monograph
Treatment Overview for Overactive Bladder
Background on Overactive Bladder (OAB)
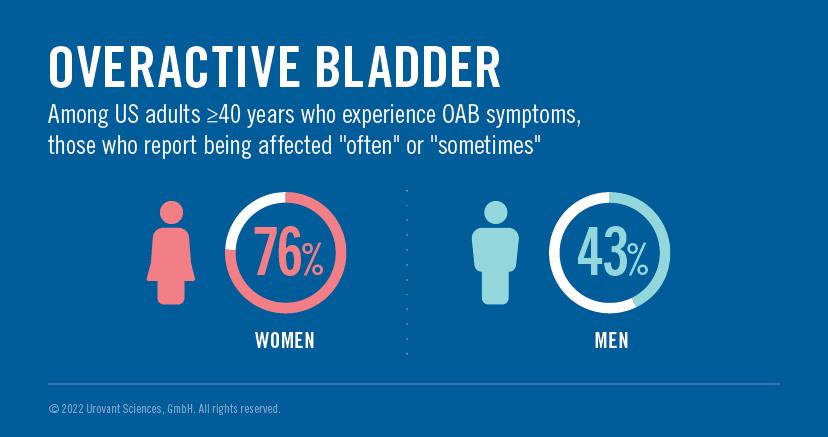
The overall prevalence of OAB in the United States among adults ≥40 years has been estimated to be 23%. Of that group, approximately 76% of women and 43% of men report being affected “often” or “sometimes.” (Figure 1) Prevalence has been found to increase with age.1 Despite this, there is a significant gap between the number of people suffering from this condition and those who ultimately seek medical advice or treatment.2,3 Additionally, even with at-risk populations, medical professionals often do not proactively inquire about urinary symptoms.2 Nonetheless, overactive bladder contributes greatly to social stigma, lower quality of life, and reduced productivity and engagement in life.4 Thus, increasing awareness among patients and healthcare providers is critically important.
It should be recognized that overactive bladder (OAB) is a syndrome consisting of typical symptoms of urinary urgency, increased daytime frequency, nocturia, and urge urinary incontinence (UUI). There are many medical diagnoses associated with overactive bladder symptoms, but OAB is fundamentally an idiopathic condition. In general, OAB occurs when the detrusor muscle experiences frequent involuntary contractions associated with increased activation of the parasympathetic nervous system. This is modulated by heightened stimulation of muscarinic neuronal receptors and subsequent acetylcholine leakage from the parasympathetic nerve terminal. This causes relative overactivity of the detrusor muscle and the accompanying urinary urgency sensation.
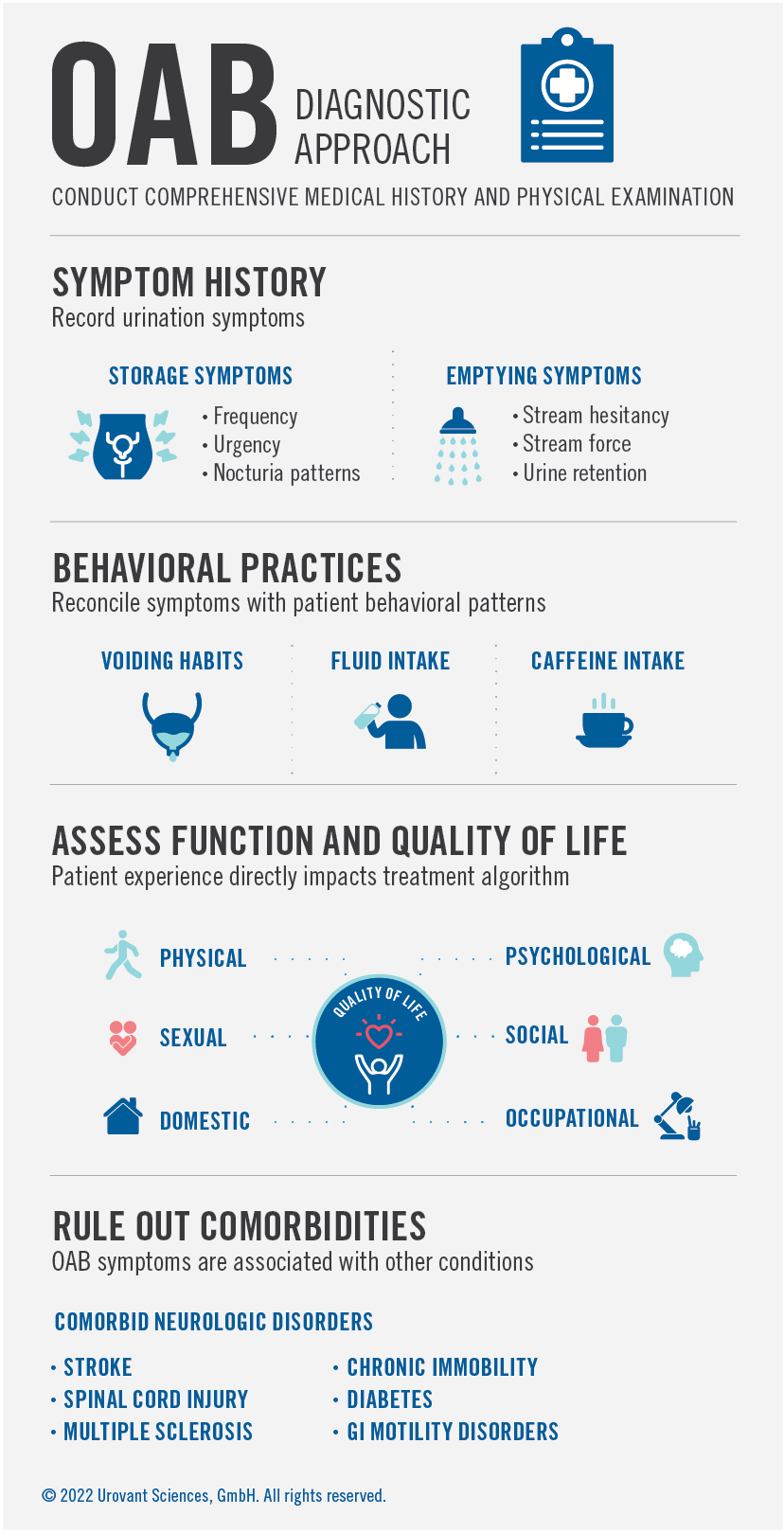
Although OAB is very common, the American Urological Association/Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (AUA/SUFU) guidelines recommend that a complete diagnostic approach be utilized to ensure that another treatable medical condition is not the cause of the patient’s urinary symptoms.5 This approach includes both comprehensive medical history-taking and a physical examination. (Figure 2) The medical history should include questions about urine storage symptoms, including frequency, urgency, and nocturia patterns, and bladder-emptying symptoms, including stream hesitancy, stream force, and urine retention. Clinicians should reconcile these symptoms with the patient’s behavioral practices, including voiding habits, daily fluid intake, and caffeine intake. This questioning should also capture the degree to which the urinary symptoms impact the patient’s daily functioning, productivity, and overall quality of life. This comprehensive picture of the patient’s experience will directly impact the subsequent treatment algorithm.
Since idiopathic OAB symptoms are associated with other organic conditions, it is critical for clinicians to inquire about and be aware of comorbid neurologic disorders (e.g., stroke, spinal cord injury, multiple sclerosis), chronic immobility, diabetes, GI motility disorders, pelvic or vaginal surgery, recurrent UTIs, or a history of pelvic radiation therapy. A comprehensive physical examination, including abdominal, genitourinary, and rectal assessments, should be completed. Finally, a cognitive examination is advisable, since this can impact some of the behavioral and pharmacologic treatment choices, particularly in the elderly population. The Mini- Mental State Examination (MMSE)6 or the Montreal Cognitive Assessment (MoCA)7,8 would be reasonable options for in-clinic cognitive examinations.
Depending on the patient specifics, additional diagnostic testing, such as urinalysis, urine culture, and a post-void residual (PVR) urine test may be helpful to assess the cause of urinary symptoms.5 Bladder diaries to be completed at home can also be useful to better understand the impact on a patient’s lifestyle and behavior; these diaries can also play a role in the eventual treatment recommendations. In general, more advanced diagnostics, including urodynamic testing, cystoscopy, and ultrasound imaging, are not indicated for uncomplicated OAB, although this should be left to the physician’s discretion.5

First-Line Treatment of Idiopathic OAB
Behavioral and Lifestyle Approaches
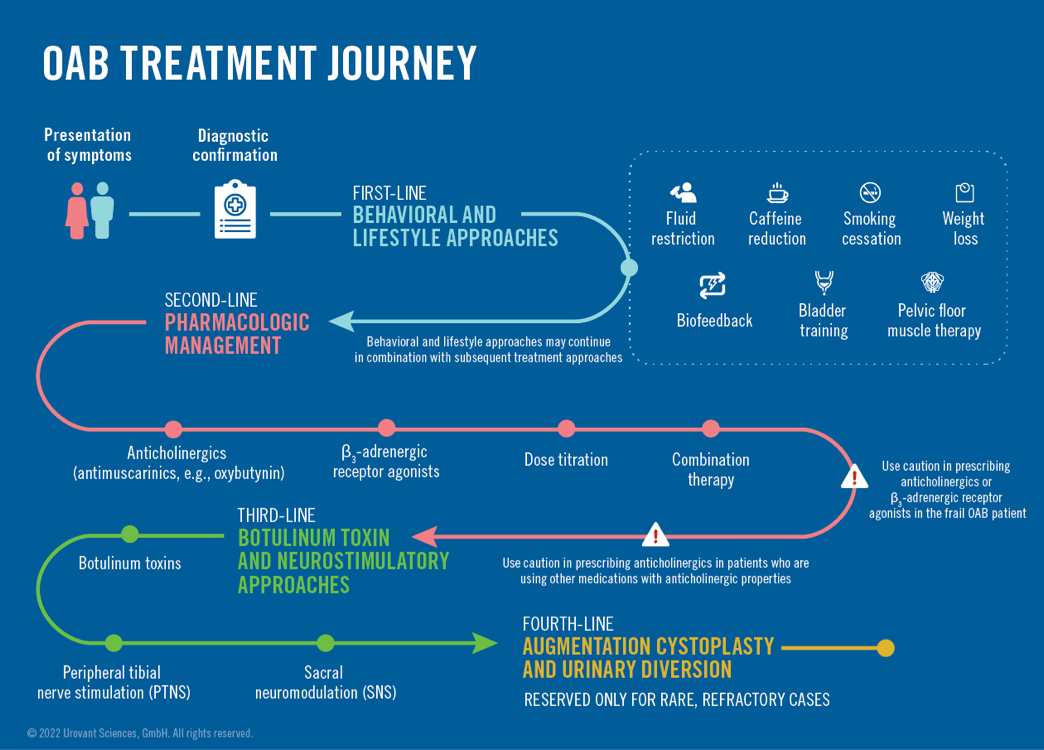
If a treatable, primary cause of the patient’s urinary symptoms are identified, then the primary treatment should focus on the management of that medical condition. If the patient is deemed to have idiopathic OAB, then the treatment algorithm begins with behavioral and lifestyle techniques, followed by pharmacologic options. The AUA/SUFU guidelines stress that providers should always weigh the benefit-risk ratio for the various treatment lines and should counsel patients about the expectations of the therapy for acceptable symptom control.5 Every treatment approach should be individualized. (Figure 4)
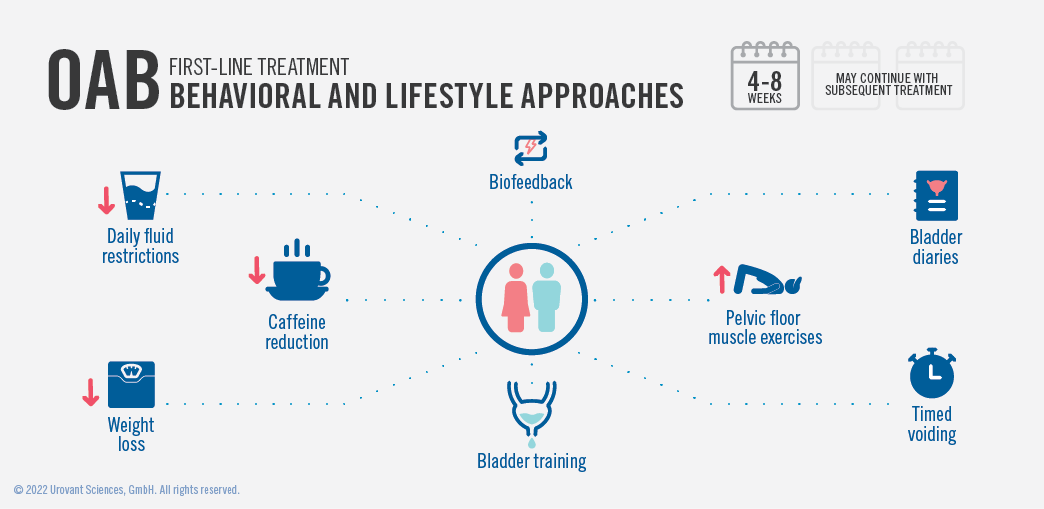
The first-line treatment for idiopathic OAB targets behavioral techniques and lifestyle adjustments. For some patients, fluid intake management or restriction, a reduction in caffeine, and weight loss can be helpful. Daily fluid restrictions of 25%, coupled with reductions in caffeine intake, have successfully reduced urinary symptoms in some patients.9 Additionally, in a study by Subak et al., weight loss interventions over six months were shown to have positive impacts on reducing the weekly number of incontinence episodes, as found in the primary intervention study group, which achieved a mean 8% weight loss.10 Bladder diaries can be an important tool in these approaches since daily insights can entrain enduring behaviors to improve urinary control. Additionally, bladder diaries allow for baseline metrics on fluid intake, caffeine use, and weight to be established as comparators. Smoking cessation programs can also be beneficial in patients for whom smoking is an important variable.
Behavioral techniques for OAB management include bladder training, pelvic floor muscle therapy, and biofeedback. Bladder training is a formal program that teaches timed voiding every 3-4 hours, along with the use of relaxation and distraction techniques to progressively delay voiding at the onset of urge sensations.11 The goal of this technique is to maximally reestablish a patient’s voluntary control over voiding, if possible. Pelvic floor muscle therapy focuses on physical exercises to improve the ability of the patient to voluntarily inhibit the contraction of the detrusor muscle.11 Biofeedback approaches can also be assistive in this approach, using electrodes placed in the abdominal and pelvic region to help patients contract their pelvic floor muscles.11,12 These approaches rely on robust patient participation and engagement, and are best used in combination. The AUA/SUFU guidelines thus recommend attempting a combination of behavioral and lifestyle approaches as the first-line therapy for patients with idiopathic OAB.5 These approaches should be attempted for a minimum of 4-8 weeks before moving to the next line of therapy, which would include pharmacologic options. It should also be noted that even if patients are deemed as candidates for pharmacologic therapy, this approach works best in conjunction with continued behavioral approaches. Multiple studies have shown that these behavioral techniques in combination with pharmacologic therapy lead to fewer incontinence episodes when compared with pharmacologic or single behavioral intervention alone.13,14
Second-Line Treatment of Idiopathic OAB
Pharmacologic Management

Anticholinergic Medications
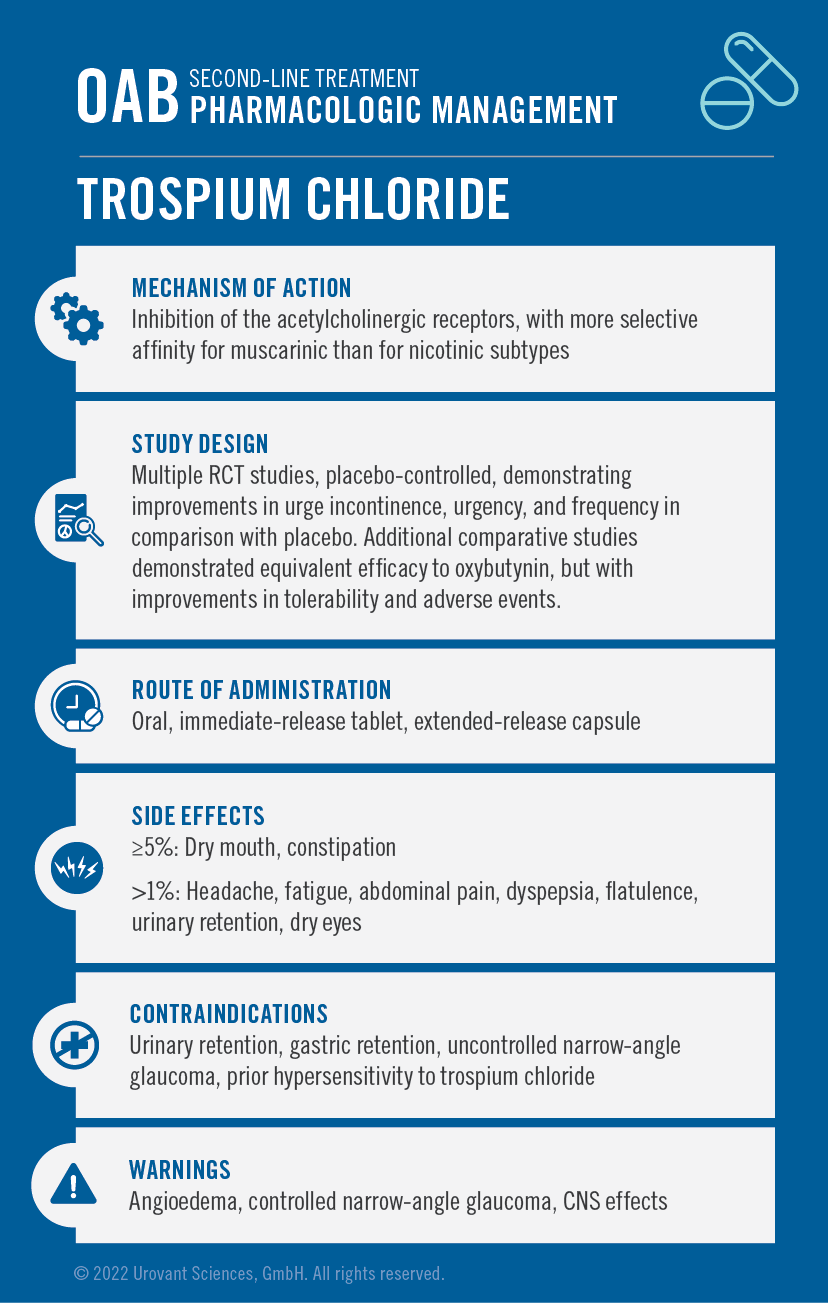
If behavioral and lifestyle interventions are not fully successful, there are multiple lines of pharmacologic treatments that can be used adjunctively. Historically, anticholinergic (antimuscarinic) medications served as the primary options for most patients with OAB. These medications specifically act through the muscarinic pathway, inhibiting the involuntary detrusor muscle contractions that are felt to be a source of OAB symptoms. There are many anticholinergic medications available (including trospium, darifenacin, fesoterodine, solifenacin, tolterodine, and oxybutynin), although oxybutynin and tolterodine are the most used in practice in the United States.11 This category of therapy has been studied in many randomized controlled trials, with moderate efficacy demonstrated in terms of both reduced episodes of urge incontinence and voids.15 Analyzed as a class, these therapies have been shown to reduce urge incontinence by 1.73 episodes per day and urinary voids by 2.06 episodes per day, from 2.79 and 11.28 at baseline, respectively. Placebo arms showed lesser reductions of daily urge incontinence by 1.06 and void episodes by 1.2 per day.15 Studies have also demonstrated no consistent differences in efficacy across the various individual medications in the anticholinergic class.16,17 One of the most commonly used medications in this class, oxybutynin (Table 1), is available in multiple formulations, including extended-release and transdermal preparations to improve compliance. Newer medications in this class, such as trospium (Table 2), may have lesser side effects than the older agents, while retaining the same degree of effectiveness. Some of these medications (trospium, darifenacin) are felt to have less blood-brain barrier penetration, thus potentially reducing the impact on CNS side effects. These newer medications also come in multiple formulations, including extended-release versions.
Despite their class efficacy, these medications have well-known and undesirable side effects due to their broad anticholinergic action; this includes dry mouth and constipation, which often limit patient satisfaction with the therapy. In comparative studies, oxybutynin has been found to have statistically significant higher rates of dry mouth and constipation in comparison with tolterodine.5 However, all the medications in this class possess high self-reported rates of dry mouth (20%-40%) and constipation (7%-9%). It should be noted that the extended-release versions (oxybutynin and tolterodine) and transdermal preparations (oxybutynin) appear to have slightly lower rates of these side effects while maintaining the same efficacy.5,18
In addition to the typical anticholinergic side effects, it is important to recognize that this medication class has also been increasingly associated with an increased risk of cognitive impairment, particularly in the aging population.19,20 This is especially salient since this population of patients is at heightened risk for OAB and commonly takes medications that may have interactions with anticholinergic agents.19,21,22 Additionally, several case-control and cohort studies have found a heightened risk of a dementia diagnosis in patients who have taken medications from the anticholinergic class.23,24,25,26,27 Although these studies do not establish a causative relationship, this body of evidence does raise caution regarding the use of these medications in patients at risk for cognitive or memory impairment. Although not entirely contraindicated, the muscarinic antagonists (anticholinergics) do carry a warning for use in the elderly population, and thus CNS effects should be monitored in any patient starting or increasing the dose of one of these types of medication.

Beta-3 Adrenergic Agonist Medications
In contrast with the older anticholinergic class of medications, two newer therapies have been approved by the FDA for the treatment of OAB that act as beta-3 adrenergic receptor agonists. These medications (mirabegron and vibegron) act by actively relaxing the detrusor smooth muscle during the storage phase of the bladder, thereby increasing fill capacity. Both medications appear to have superior efficacy compared with placebo, as well as comparable efficacy with fewer adverse events when compared with anticholinergic treatments. The first of these medications, mirabegron (Table 3), was approved by the FDA in 2012, and is indicated as monotherapy for OAB or in combination with the anticholinergic medication solifenacin succinate (refer to mirabegron label30). In a study by Herschorn et al., two strengths of mirabegron were used (25 mg or 50 mg daily) in comparison with placebo over 12 weeks. The mirabegron treatment arms decreased daily incontinence episodes by 1.36 (25 mg) and 1.38 (50 mg) compared to 0.96 in the placebo group, and daily micturitions decreased by 1.65 (25 mg) and 1.60 (50 mg) in the treatment arms vs only 1.18 for the placebo arm, with both active arms reaching statistical significance.31
The mirabegron trials were associated with treatment-emergent side effects, but they appear to be less in comparison with anticholinergic medications. For mirabegron, a study by Chapple et al. showed lower rates of dry mouth vs tolterodine.32 Additionally, because of mirabegron’s mechanism of action and its low potential for crossing the blood-brain barrier, there is lower risk for CNS side effects as compared with the anticholinergic medications. Hypertension is one of the more common adverse events associated with mirabegron as compared with placebo (11.3% vs 7.6%)30; currently, mirabegron does carry a warning and is not recommended for patients with severe uncontrolled hypertension. The most common adverse events in the mirabegron trials were hypertension, nasopharyngitis, urinary tract infection, and headache (all >2% and greater than the placebo arms).
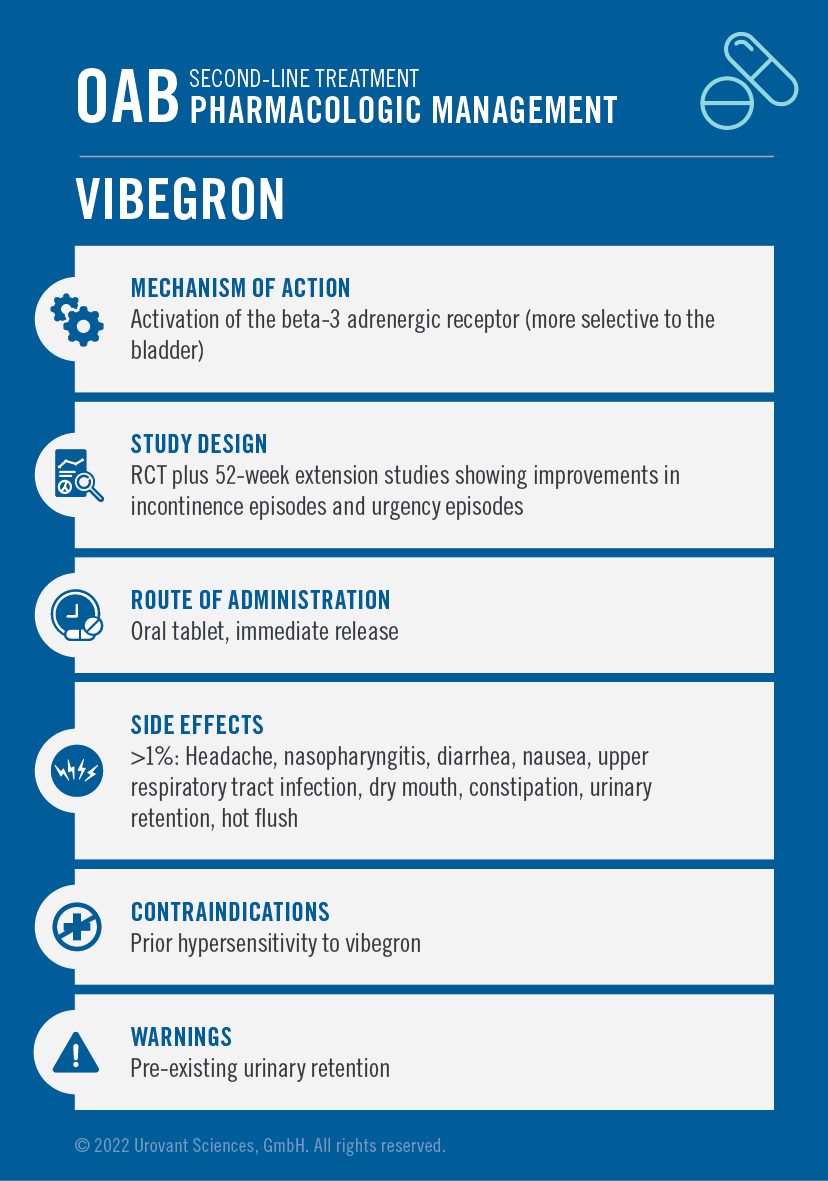
A second selective beta-3 adrenergic agonist, vibegron (Table 4), was also approved by the FDA in 2020 for the treatment of OAB, based on data from multiple randomized controlled trials. A pivotal 12-week treatment trial vs placebo demonstrated statistically significant improvements in both daily voids (p< 0.001) and urge incontinence episodes (p< 0.0001) at 12 weeks.33 A subsequent phase 3 study of once-daily vibegron vs active control was completed with a primary outcome focused on safety, as measured by the incidence of adverse events. No clinically meaningful differences in adverse events were found between the treatment groups in the study. This 52-week extension analysis also demonstrated greater improvements in urinary incontinence episodes, urinary episodes, and total incontinence episodes, which were secondary endpoints in the study. In comparing the two treatment arms, 61% of patients on vibegron experienced a ≥75% reduction in urge urinary incontinence episodes vs 54% for patients on active control.34
The primary adverse events reported for vibegron vs placebo were headache (4.0% vs 2.4%), nasopharyngitis (2.8% vs 1.7%), diarrhea (2.2% vs 1.1%), and nausea (2.2% vs 1.1%). The incidence of hypertension in the primary vibegron trial at 12 weeks was equal to that of placebo (1.7% vs 1.7%).33 In the 52-week extension study for vibegron, the incidence of hypertension was 8.8% but this was comparable to the group of patients taking active control (8.6%). At the end of the trial, the mean changes in blood pressure were not statistically different from baseline in the treatment cohort.34 These studies, together with approximately five years of cumulative postmarketing experience for vibegron (data on file), show that hypertension is not considered an adverse drug reaction (ADR) for vibegron.
Medication Combinations
If individual medications are not fully effective and the patient desires a more aggressive approach, combinations of anticholinergics and beta-3 adrenergic agonists can also be attempted. In particular, the combination of solifenacin and mirabegron has been studied in comparison with placebo, mirabegron in monotherapy, and solifenacin in monotherapy.35,36,37 These studies demonstrated stronger effect sizes for the combination arms in terms of both urge incontinence and voiding episodes. Perhaps as expected, however, the combination therapies also exhibited a higher rate of adverse events (49%), including dry mouth and constipation, as compared with either of the monotherapy arms (41% for mirabegron and 44% for solifenacin).37 Despite these findings, for a motivated patient with refractory symptoms, a combination approach may be warranted. It is again noted that if anticholinergic medications are included, clinicians should consider either extended-release or transdermal formulations, which have been shown to carry fewer side effects with the same degree of clinical effectiveness.
Special Considerations
As mentioned earlier, given the potential for impact on cognitive functioning, anticholinergic treatment options should be used cautiously or avoided in the elderly, patients with pre-existing cognitive impairment, and patients who are taking other medications with anticholinergic properties. Even though a trial of an anticholinergic medication is recommended through guidelines, a decision should be made between the clinician, patient, and caregivers with consideration of the benefit-risk balance. If an anticholinergic trial is pursued in these patient populations, a low dose should be employed first, with regular monitoring of cognitive functioning.
Additionally, for all patient populations, it must be recognized that commitment to a long-term treatment approach is a critical element of success. For both behavioral and pharmacologic techniques, it requires habit-forming and patience to make incremental improvements and improve health outcomes.2,39 Unfortunately, for many patients with OAB symptoms, maintaining a persistent therapy is often challenging. Unmet treatment expectations, medication switches, and side effects are some of the key reasons behind this.40 Therefore, clinicians should always ensure that patients have a realistic expectation and plan for their long-term OAB treatment approach.
Third-Line Treatment of Idiopathic OAB
Botulinum Toxin and Neurostimulatory Approaches

For selected patients who have intractable symptoms and have not responded to earlier therapeutic lines, onabotulinumtoxinA injections (Table 5) have also been approved by the FDA and can be considered. Botulinum toxin works by inhibiting the release of acetylcholine from presynaptic nerve terminals, thus preventing bladder detrusor muscle activity. This procedurally involves direct intradetrusor bladder injections performed under local anesthesia via cystoscopy. In clinical trials, compared with anticholinergics and mirabegron, onabotulinumtoxinA injections were also shown to decrease the number of daily incontinence and urgency episodes.41 Placebo-controlled studies of botulinum toxin injections also demonstrated a benefit on the number of daily incontinence episodes.42 However, long-term follow studies on the use of botulinum toxin injections show a high rate of discontinuation, primarily due to intolerability of the procedure (43%) and lack of sufficient efficacy (27%).43
Neurostimulation therapy has also been studied as a potential option for some patients with intractable OAB symptoms. Percutaneous tibial nerve stimulation (PTNS) and transcutaneous tibial nerve stimulation (TTNS) are two approaches based on the concept that peripheral nerve stimulation may impact bladder functioning. PTNS involves an office-based procedure in which a small needle is used to administer a mild electrical stimulation behind the ankle for 30 minutes, usually with 12 weeks of sessions. This procedure has been shown in systematic reviews to improve symptoms in some patients against placebo,5 although head-to-head trials in comparison with traditional anticholinergics did not show evidence of superiority.44 Sacral neuromodulation is another FDA-approved procedure in which a small neurostimulator is surgically implanted after testing the patient for candidacy. Studies have demonstrated that between 56% and 68% of intractable patients have at least a 50% improvement in urinary incontinence episodes and urinary frequency45,46; however, this procedure is invasive, and a relatively high percentage of patients may require revision or replacement of the device.47 Thus, this therapy should only be considered for refractory patients with continuing symptoms that severely impact quality of life.
Fourth-Line Treatment of Idiopathic OAB
Surgical Approaches
The final category of therapies for intractable OAB patients involves primary surgical solutions. It is stressed that these approaches are only for rare refractory and complicated patients who have attempted many prior lines of treatment. Augmentation cystoplasty, in which a portion of bladder is replaced by a bowel segment to make it larger, is a procedure that the AUA guidelines recommend only in patients with refractory neurogenic OAB and with poor compliance to pharmacotherapy. Urinary diversion is another surgical procedure in which an alternative pathway for urine release is created due to blockage of the body’s natural anatomy. It is noted that indwelling catheters are not recommended due to risk of adverse events, except in rare patient situations.
References
- Coyne KS, Sexton CC, Vats V, Thompson C, Kopp ZS, Milsom I. National community prevalence of overactive bladder in the United States stratified by sex and age. Urology. 2011;77(5):1081-1087.
- Leron E, Weintraub AY, Mastrolia SA, Schwarzman P. Overactive bladder syndrome: evaluation and management. Curr Urol. 2017;11:117-125.
- Benner JS, Becker R, Fanning K, et al. Bother related to bladder control and health care seeking behavior in adults in the United States. J Urol. 2009;181(6):2591-2598.
- Burgio KL, Locher JL, Goode PS, et al. Behavioral vs drug treatment for urge urinary incontinence in older women: a randomized controlled trial. JAMA. 1998;280(23):1995-2000.
- Gormley EA, Lightner DJ, Burgio KL, et al. Diagnosis and treatment of non-neurogenic overactive bladder (OAB) in adults: an AUA/SUFU guideline (2019). American Urological Association. Available at: https://www.auanet.org/guidelines/guidelines/overactive-bladder-(oab)-guideline. Accessed June 23, 2022.
- Folstein MF, Robins LN, Helzer JE. The mini-mental state examination. Arch Gen Psychiatry. 1983;40(7):812.
- Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. JAGS. 2005;53:695-699.
- De Roeck EE, De Deyn PP, Dierckx E, Engelborghs S. Brief cognitive screening instruments for early detection of Alzheimer’s disease: a systematic review. Alzheimer’s Res Ther. 2019:11(21):1-14.
- Bryant CM, Dowell CJ, Fairbrother G. Caffeine reduction education to improve urinary symptoms. Br J Nurs. 2002;11(8):560-565.
- Subak LL, Wing R, West DS, et al. Weight loss to treat urinary incontinence in overweight and obese women. N Engl J Med. 2009;360(5):481-490.
- Ellsworth PI, Kim ED. Overactive bladder [WebMD Medscape website]. January 21, 2021. Available at: https://emedicine.medscape.com/article/459340-overview#a5. Accessed June 24, 2022.
- Lukacz, ES. Urgency urinary incontinence/overactive bladder (OAB) in females: treatment. 2021. [UpToDate website]. UpToDate, Inc. Accessed June 3, 2022.
- Burgio KL, Locher JL, Goode PS. Combined behavioral and drug therapy for urge incontinence in older women. J Am Geriatr Soc. 2000;48(4):370-374.
- Burgio KL, Kraus SR, Johnson TM, et al. Effectiveness of combined behavioral and drug therapy for overactive bladder symptoms in men: a randomized clinical trial. JAMA Intern Med. 2020;180(3):411-419.
- Reynolds WS, McPheeters M, Blume J, et al. Comparative effectiveness of anticholinergic therapy for overactive bladder in women: a systematic review and meta-analysis. Obstet Gynecol. 2015;125(6):1423-1432.
- Chapple CR, Khullar V, Gabriel Z, Muston D, Bitoun CE, Weinstein D. The effects of antimuscarinic treatments in overactive bladder: an update of a systematic review and meta-analysis. Eur Urol. 2008;54(3):543-562.
- Khullar V, Chapple C, Gabriel Z, Dooley JA. The effects of antimuscarinics on health-related quality of life in overactive bladder: a systematic review and meta-analysis. Urology. 2006;68(2 Suppl):38-48.
- Dmochowski RR, Sand PK, Zinner NR, Gittelman MC, Davila GW, Sanders SW. Comparative efficacy and safety of transdermal oxybutynin and oral tolterodine versus placebo in previously treated patients with urge and mixed urinary incontinence. Urology. 2003;62(2):237-242.
- Andre L, Gallini A, Montastruc F, et al. Association between anticholinergic (atropinic) drug exposure and cognitive function in longitudinal studies among individuals over 50 years old: a systematic review. Eur J Clin Pharmacol. 2019;75(12):1631-1644.
- Panel AGSBCUE, Fick DM, Semla TP, et al. American Geriatrics Society 2019 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2019;67(4):674-694.
- Gray SL, Anderson ML, Dublin S, et al. Cumulative use of strong anticholinergics and incident dementia: a prospective cohort study. JAMA Intern Med. 2015;175(3):401-407.
- Wang Y-C, Chen Y-L, Huang C-C, et al. Cumulative use of therapeutic bladder anticholinergics and the risk of dementia in patients with lower urinary tract symptoms: a nationwide 12-year cohort study. BMC Geriatrics. 2019;19:380.
- Yoshida M, Kato D, Nishimura T, Van Schyndle J, Uno S, Kimura T. Anticholinergic burden in the Japanese elderly population: use of antimuscarinic medications for overactive bladder patients. Int J Urol. 2018;25(10):855-862.
- Green AR, Reifler LM, Boyd CM, Weffald LA, Bayliss EA. Medication profiles of patients with cognitive impairment and high anticholinergic burden. Drugs Aging. 2018;35(3):223-232.
- Coupland CAC, Hill T, Dening T, Morriss R, Moore M, Hippisley-Cox J. Anticholinergic drug exposure and the risk of dementia: a nested case-control study. JAMA Intern Med. 2019;179(8):1084-1093.
- Hanlon P, Quinn TJ, Gallacher KI, et al. Assessing risks of polypharmacy involving medications with anticholinergic properties. Ann Fam Med. 2020;18(2):148-155.
- Welk B, McArthur E. Increased risk of dementia among patients with overactive bladder treated with an anticholinergic medication compared to a beta-3 agonist: a population-based cohort study. BJU Int. 2020;126(1):183-190.
- DITROPAN XL® (oxybutynin chloride) [prescribing information]. Titusville, NJ: Janssen Pharmaceuticals, Inc.; 2016.
- SANCTURA® (trospium chloride) [prescribing information]. Irvine, CA: Allergan, Inc.; 2012.
- MYRBETRIQ® (mirabegron) [prescribing information]. Northbrook, IL: Astellas Pharma US, Inc.; 2018.
- Herschorn S, Barkin J, Castro-Diaz D, et al. A phase III, randomized, double-blind, parallel-group, placebo-controlled, multicentre study to assess the efficacy and safety of the β3 adrenoceptor agonist, mirabegron, in patients with symptoms of overactive bladder. Urology. 2013;82:313-20.
- Chapple CR, Kaplan SA, Mitcheson D, et al. Randomized double-blind, active-controlled phase 3 study to assess 12-month safety and efficacy of mirabegron, a β3-adrenoceptor agonist, in overactive bladder. Eur Urol. 2013;63(2):296-305.
- Staskin D, Frankel J, Varano S, Shortino D, Jankowich R, Mudd PN Jr. International phase III, randomized, double-blind, placebo and active controlled study to evaluate the safety and efficacy of vibegron in patients with symptoms of overactive bladder: EMPOWUR. J Urol. 2020:204:316-324.
- Staskin D, Frankel J, Varano S, Shortino D, Jankowich R, Mudd PN Jr. Once-daily vibegron 75 mg for overactive bladder: long-term safety and efficacy from a double-blind extension study of the international phase 3 trial (EMPOWUR). J Urol. 2021;205(5):1421-1429.
- Herschorn S, Chapple CR, Abrams P, et al. Efficacy and safety of combinations of mirabegron and solifenacin compared with monotherapy and placebo in patients with overactive bladder (SYNERGY study). BJU Int. 2017;120(4):562-575.
- Drake MJ, Chapple C, Esen AA, et al. Efficacy and safety of mirabegron add-on therapy to solifenacin in incontinent overactive bladder patients with an inadequate response to initial 4-week solifenacin monotherapy: a randomised double-blind multicentre phase 3B study (BESIDE). Eur Urol. 2016;70(1):136-145.
- Gratzke C, van Maanen R, Chapple C, et al. Long-term safety and efficacy of mirabegron and solifenacin in combination compared with monotherapy in patients with overactive bladder: a randomised, multicentre phase 3 study (SYNERGY II). Eur Urol. 2018;74(4):501-509.
- GEMTESA® (vibegron) [prescribing information]. Irvine, CA: Urovant Sciences, Inc.; 2020.
- Krueger KP, Berger BA, Felkey B. Medication adherence and persistence: a comprehensive review. Adv Ther. 2005;22(4):313-356.
- Benner JS, Nichol MB, Rovner ES, et al. Patient‐reported reasons for discontinuing overactive bladder medication. BJU Int. 2010;105(9):1276-1282.
- Drake MJ, Nitti VW, Ginsberg DA, et al. Comparative assessment of the efficacy of onabotulinumtoxinA and oral therapies (anticholinergics and mirabegron) for overactive bladder: a systematic review and network meta‐analysis. BJU Int. 2017;120(5):611-622.
- Cui Y, Wang L, Liu L, et al. Botulinum toxin-A injections for idiopathic overactive bladder: a systematic review and meta-analysis. Urol Int. 2013;91(4):429-438.
- Marcelissen TAT, Rahnama’i M, Snijkers A, Schurch B, De Vries P. Long-term follow-up of intravesical botulinum toxin-A injections in women with idiopathic overactive bladder symptoms. World J Urol. 2017;35(2):307-311.
- Burton C, Sajja A, Latthe P. Effectiveness of percutaneous posterior tibial nerve stimulation for overactive bladder: a systematic review and meta‐analysis. Neurourol and Urodyn. 2012;31(8):1206-1216.
- Janknegt RA, Hassouna MM, Siegel SW, et al. Long-term effectiveness of sacral nerve stimulation for refractory urge incontinence. Eur Urol. 2001;39(1):101-106.
- Siegel SW, Catanzaro F, Dijkema HE, et al. Long-term results of a multicenter study on sacral nerve stimulation for treatment of urinary urge incontinence, urgency-frequency, and retention. Urology. 2000;56(6 Suppl 1):87-91.
- Noblett K, Benson K, Kreder K. Detailed analysis of adverse events and surgical interventions in a large prospective trial of sacral neuromodulation therapy for overactive bladder patients. Neurourol and Urodyn. 2017;36(4):1136-1139.
- BOTOX® (onabotulinumtoxinA) [prescribing information]. Irvine, CA: Allergan, Inc.; 2017.
